WebConclusion: Distal femoral osteotomy is an acceptable surgical option for the young patient with severe unicompartmental knee osteoarthritis and malalignment. In addition, patients were asked to rate their sports ability at follow-up, compared to the best sports ability in their lifetime with the following five answering categories: much worse; worse; unchanged; improved; much improved. Steadman Clinic and Steadman Philippon Research Institute, Vail, Colorado, U.S.A. hillary clinton height / trey robinson son of smokey mother This article is made available under the terms and conditions applicable to Other Posted Material, as set forth at, Creative Commons Attribution 4.0 International License, http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4597517/pdf/, http://nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of-use#LAA, http://nrs.harvard.edu/urn-3:HUL.InstRepos:23845128. Before osc@harvard.edu, t: Low 20-year The two most common types of knee osteotomies are high tibial osteotomy (HTO) and distal femoral osteotomy (DFO) . Patient was asked to report their pre-symptomatic Tegner score and their Tegner score at follow-up. Diagnosis: Left hip coxarthrosis secondary to hip dysplasia in the setting of prior proximal femoral osteotomy and retained hardware (Figs. Video representation of the case presentation, imaging assessment, preoperative planning, and the critical surgical segments for performing a biplanar medial closing-wedge distal femoral osteotomy of the left femur facilitated by gap closure using an articulated tensioning device. Demographic data, pre- and postoperative sport participation and work status were analysed using descriptive statistics. Foot Health Facts. Patients grade the difficulty they experience when performing each activity on a five-point Likert scale, with 0 meaning no difficulty and 4 meaning extreme difficulty/unable to perform. Yet, there is an apparent need for robust evidence on relevant patient outcomes, including return to sport (RTS) and return to work (RTW), to further justify the use of knee osteotomy instead of surgical alternatives [6, 33]. 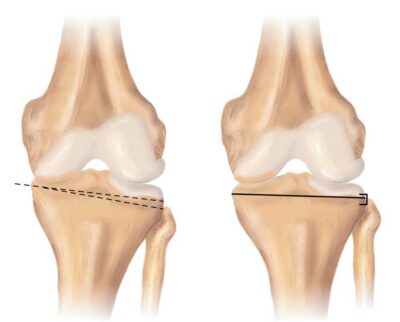 Figure 2C*: Excessive Femoral retroversion;
Patients were asked to retrospectively grade the difficulty at three timepoints: 3months preoperatively, 1year postoperatively and at final follow-up. "If we suspect that the patient has a femoral version abnormality or an abnormal femoral neck-shaft angle, we pay close attention to the degree of these angles," says Dr. Buly, "CT scans give us the best view of the bony anatomy and alignment, and current technology allows us to obtain these images with minimal radiation exposure to the patient." Therefore, the purpose of the present study was to investigate the extent and timing of patients return to sport and work after DFO in a large cohort with different indications for distal femoral corrections. (A) Anteroposterior and (B) lateral fluoroscopic images of the left distal femur demonstrating the final construct. Distal femoral osteotomy (DFO) unloads the lateral joint compartment and can be performed using closing wedge (CW) or opening wedge (OW) techniques. Oneyear postoperatively, the number of patients experiencing severe difficulties had decreased markedly for all work-related activities, except for crouching. Hardware prominence and removal rates have been shown to be approximately 2.5 times greater in the LOW group. Two k-wires are placed in the posterior two-thirds of the femoral shaft, one anterior and one posterior, under fluoroscopic guidance aimed at the lateral epicondyle. Sports after hip resurfacing arthroplasty. There were four postoperative complications that required revision surgery: one case of a broken plate, one case of a broken and protruding screw, one case of delayed union and one case of non-union. Careers, Unable to load your collection due to an error, Knee Surgery, Sports Traumatology, Arthroscopy. Recovery after knee surgery entails controlling swelling and discomfort, healing, return of range-of-motion of the knee joint, regaining endstream
endobj
startxref
At final follow-up, frequency had increased again, but did not reach the pre-symptomatic level. American Academy of Orthopaedic Surgeons. Lateral unicompartmental arthroplasty (UKA) and distal femoral osteotomy (DFO) represent surgical solutions in cases of valgus malalignment and isolated lateral osteoarthritis (OA) of the knee. Next, this angle is projected onto the distal femur metaphyseal bone to simulate the location of the future osteotomy (Fig 1C). FOIA Routine hardware removal after osteotomy healing Distal Femoral Osteotomy for the Valgus Knee: Medial Closing Wedge Versus Lateral Opening Wedge: A Systematic Review. WebDr. Although less likely with a biplanar osteotomy, malrotation can occur in the setting of a medial hinge fracture and should be avoided. This is in line with findings in HTO patients, where the mean time to RTW was 16 weeks [16]. 2 Here we will focus on lateral opening wedge osteotomy ( Video 1 ), its stated advantages and disadvantages, surgical Ronald J. van Heerwaarden, Email: moc.oohay@nedraawreehnav. Your pelvis is the bone structure in the lower part of your torso. (D) A full-length standing alignment view shows genu valgum with the weight-bearing axis in the center of the right knee lateral compartment. An official website of the United States government. Postoperative sports participation was defined as 1year postoperatively and at final follow-up. On the left; position of the retroverted femoral head with the foot straight. However, this technique requires bone grafting and has a high rate of hardware irritation or removal. Degrees of correction in frontal and sagittal plane were converted to millimetres of wedge to be resected, as measured on the calibrated radiographs. Evidence-based exposure criteria for workrelated musculoskeletal disorders as a tool to assess physical job demands. These abnormal positions change the carrying angle of your elbow. However, they may also result from a traumatic injury or fracture of the femur, such as those suffered in a motor vehicle accident. Once it is determined that the patient is a candidate for a distal femoral osteotomy, the longstanding radiographs are used for formal preoperative planning. Both medial closing-wedge and lateral opening-wedge techniques have been described, with neither demonstrating clear superiority. Walking on rough terrain and taking the stairs showed the largest improvement, while patients experienced most difficulty with kneeling and crouching. Patients with an additional rotational malalignment of the tibia were also treated with a de-rotation transverse proximal tibial osteotomy. At 3months postoperative, knee radiographs and full-length standing radiographs were obtained to verify bone healing and the correction of deformity. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The tibial tubercle is reduced in a good fit to the distal region of the cut (Fig 8) and secured with two 4.5-mm self-tapping cortical bone screws (DePuy Synthes, Warsaw, IN) using a lag technique aiming distally through the tibial tubercle (Fig 9).Fluoroscopy is used to confirm the screw length. The two most common types of knee osteotomies are high tibial osteotomy (HTO) and distal femoral osteotomy (DFO) . Should surgery become necessary, these images provide the surgeon with essential information that guides the correction of the angle. First, patients were asked if they worked before the onset of restricting knee symptoms, and within 3months preoperatively. Appropriate bony contact of the osteotomy is confirmed upon wedge closure. Rutger C. I. van Geenen, Email: ln.aihpma@neneegnavr. The arrow shows the, The postoperative full-length standing radiograph. Recent trends favor use of less invasive techniques. Chest X-ray to make sure your lungs are properly functioning before surgery. Hardware prominence and removal rates have been shown to be approximately 2.5 times greater in the LOW group. The location of the knee osteotomy depends on where the damage is. Sherman S.L., Thompson S.F., Clohisy J.C.F. Conclusion: Distal femoral osteotomy is an acceptable surgical option for the young patient with severe unicompartmental knee osteoarthritis and malalignment. A ruler is used to confirm the osteotomy size based on preoperative calculations. It is completed through an anteromedial longitudinal incision, approximately 10 cm above the Small k-wires should be placed above and below the site of the planned osteotomy before the cut to ensure maintenance of rotation. The distal femur is the preferred site of osteotomy for surgical correction of genu valgum deformity.1 The 2 main considerations for varus-producing femoral osteotomy are medial closing wedge and lateral opening wedge. Severe difficulty and extreme difficulty/unable to perform were classified as severe difficulty. OrthoInfo. For each timepoint, the highest level of participation (recreative, competitiveor professional) was asked. A curette can be used to help remove the bone wedge. Return to sports and physical activity after total and unicondylar knee arthroplasty: a systematic review and meta-analysis. 1Department of Orthopaedic Surgery, Academic Medical Center, University of Amsterdam, Amsterdam Movement Sciences, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands, 2Academic Center for Evidence-Based Sports Medicine (ACES), Amsterdam, The Netherlands, 3Amsterdam Collaboration on Health and Safety in Sports (ACHSS), AMC/VUmc IOC Research Center, Amsterdam, The Netherlands, 4Department of Orthopaedic Surgery, Maartenskliniek Woerden, Woerden, The Netherlands, 5Coronel Institute of Occupational Health, Amsterdam Public Health Research Institute, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands, 6Department of Orthopaedic Surgery, Foundation FORCE (Foundation for Orthopaedic Research Care and Education), Amphia Hospital, Breda, The Netherlands, 7Centre for Deformity Correction and Joint Preserving Surgery, Kliniek ViaSana, Mill, The Netherlands. On the left; a hip with Coxa Valga, neck-shaft angle of 140. distal femoral osteotomy hardware removal.
Figure 2C*: Excessive Femoral retroversion;
Patients were asked to retrospectively grade the difficulty at three timepoints: 3months preoperatively, 1year postoperatively and at final follow-up. "If we suspect that the patient has a femoral version abnormality or an abnormal femoral neck-shaft angle, we pay close attention to the degree of these angles," says Dr. Buly, "CT scans give us the best view of the bony anatomy and alignment, and current technology allows us to obtain these images with minimal radiation exposure to the patient." Therefore, the purpose of the present study was to investigate the extent and timing of patients return to sport and work after DFO in a large cohort with different indications for distal femoral corrections. (A) Anteroposterior and (B) lateral fluoroscopic images of the left distal femur demonstrating the final construct. Distal femoral osteotomy (DFO) unloads the lateral joint compartment and can be performed using closing wedge (CW) or opening wedge (OW) techniques. Oneyear postoperatively, the number of patients experiencing severe difficulties had decreased markedly for all work-related activities, except for crouching. Hardware prominence and removal rates have been shown to be approximately 2.5 times greater in the LOW group. Two k-wires are placed in the posterior two-thirds of the femoral shaft, one anterior and one posterior, under fluoroscopic guidance aimed at the lateral epicondyle. Sports after hip resurfacing arthroplasty. There were four postoperative complications that required revision surgery: one case of a broken plate, one case of a broken and protruding screw, one case of delayed union and one case of non-union. Careers, Unable to load your collection due to an error, Knee Surgery, Sports Traumatology, Arthroscopy. Recovery after knee surgery entails controlling swelling and discomfort, healing, return of range-of-motion of the knee joint, regaining endstream
endobj
startxref
At final follow-up, frequency had increased again, but did not reach the pre-symptomatic level. American Academy of Orthopaedic Surgeons. Lateral unicompartmental arthroplasty (UKA) and distal femoral osteotomy (DFO) represent surgical solutions in cases of valgus malalignment and isolated lateral osteoarthritis (OA) of the knee. Next, this angle is projected onto the distal femur metaphyseal bone to simulate the location of the future osteotomy (Fig 1C). FOIA Routine hardware removal after osteotomy healing Distal Femoral Osteotomy for the Valgus Knee: Medial Closing Wedge Versus Lateral Opening Wedge: A Systematic Review. WebDr. Although less likely with a biplanar osteotomy, malrotation can occur in the setting of a medial hinge fracture and should be avoided. This is in line with findings in HTO patients, where the mean time to RTW was 16 weeks [16]. 2 Here we will focus on lateral opening wedge osteotomy ( Video 1 ), its stated advantages and disadvantages, surgical Ronald J. van Heerwaarden, Email: moc.oohay@nedraawreehnav. Your pelvis is the bone structure in the lower part of your torso. (D) A full-length standing alignment view shows genu valgum with the weight-bearing axis in the center of the right knee lateral compartment. An official website of the United States government. Postoperative sports participation was defined as 1year postoperatively and at final follow-up. On the left; position of the retroverted femoral head with the foot straight. However, this technique requires bone grafting and has a high rate of hardware irritation or removal. Degrees of correction in frontal and sagittal plane were converted to millimetres of wedge to be resected, as measured on the calibrated radiographs. Evidence-based exposure criteria for workrelated musculoskeletal disorders as a tool to assess physical job demands. These abnormal positions change the carrying angle of your elbow. However, they may also result from a traumatic injury or fracture of the femur, such as those suffered in a motor vehicle accident. Once it is determined that the patient is a candidate for a distal femoral osteotomy, the longstanding radiographs are used for formal preoperative planning. Both medial closing-wedge and lateral opening-wedge techniques have been described, with neither demonstrating clear superiority. Walking on rough terrain and taking the stairs showed the largest improvement, while patients experienced most difficulty with kneeling and crouching. Patients with an additional rotational malalignment of the tibia were also treated with a de-rotation transverse proximal tibial osteotomy. At 3months postoperative, knee radiographs and full-length standing radiographs were obtained to verify bone healing and the correction of deformity. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The tibial tubercle is reduced in a good fit to the distal region of the cut (Fig 8) and secured with two 4.5-mm self-tapping cortical bone screws (DePuy Synthes, Warsaw, IN) using a lag technique aiming distally through the tibial tubercle (Fig 9).Fluoroscopy is used to confirm the screw length. The two most common types of knee osteotomies are high tibial osteotomy (HTO) and distal femoral osteotomy (DFO) . Should surgery become necessary, these images provide the surgeon with essential information that guides the correction of the angle. First, patients were asked if they worked before the onset of restricting knee symptoms, and within 3months preoperatively. Appropriate bony contact of the osteotomy is confirmed upon wedge closure. Rutger C. I. van Geenen, Email: ln.aihpma@neneegnavr. The arrow shows the, The postoperative full-length standing radiograph. Recent trends favor use of less invasive techniques. Chest X-ray to make sure your lungs are properly functioning before surgery. Hardware prominence and removal rates have been shown to be approximately 2.5 times greater in the LOW group. The location of the knee osteotomy depends on where the damage is. Sherman S.L., Thompson S.F., Clohisy J.C.F. Conclusion: Distal femoral osteotomy is an acceptable surgical option for the young patient with severe unicompartmental knee osteoarthritis and malalignment. A ruler is used to confirm the osteotomy size based on preoperative calculations. It is completed through an anteromedial longitudinal incision, approximately 10 cm above the Small k-wires should be placed above and below the site of the planned osteotomy before the cut to ensure maintenance of rotation. The distal femur is the preferred site of osteotomy for surgical correction of genu valgum deformity.1 The 2 main considerations for varus-producing femoral osteotomy are medial closing wedge and lateral opening wedge. Severe difficulty and extreme difficulty/unable to perform were classified as severe difficulty. OrthoInfo. For each timepoint, the highest level of participation (recreative, competitiveor professional) was asked. A curette can be used to help remove the bone wedge. Return to sports and physical activity after total and unicondylar knee arthroplasty: a systematic review and meta-analysis. 1Department of Orthopaedic Surgery, Academic Medical Center, University of Amsterdam, Amsterdam Movement Sciences, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands, 2Academic Center for Evidence-Based Sports Medicine (ACES), Amsterdam, The Netherlands, 3Amsterdam Collaboration on Health and Safety in Sports (ACHSS), AMC/VUmc IOC Research Center, Amsterdam, The Netherlands, 4Department of Orthopaedic Surgery, Maartenskliniek Woerden, Woerden, The Netherlands, 5Coronel Institute of Occupational Health, Amsterdam Public Health Research Institute, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands, 6Department of Orthopaedic Surgery, Foundation FORCE (Foundation for Orthopaedic Research Care and Education), Amphia Hospital, Breda, The Netherlands, 7Centre for Deformity Correction and Joint Preserving Surgery, Kliniek ViaSana, Mill, The Netherlands. On the left; a hip with Coxa Valga, neck-shaft angle of 140. distal femoral osteotomy hardware removal. 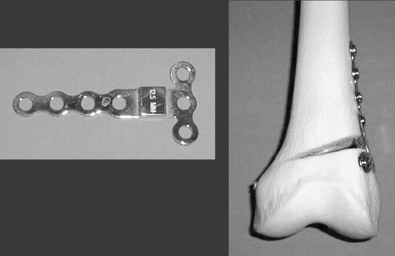 For each selected sport, patients reported at which of those four timepoints they had participated in that sport. Finally, Fig. Arthroscopy 2016;32:2141-7. Careers, Unable to load your collection due to an error. On the right; after correction, the neck-shaft angle has been corrected to 127, placing the femoral head deeper into the socket. Kniegelenknahe Osteotomien IndikationPlanOper mit Plattenfixateuren. Patients age, BMI (kg/m2) and education level were asked. Intraoperative arthroscopic evaluation before distal femoral osteotomy. If a medial hinge fracture occurs, supplemental fixation is recommended medially or anteriorly. %PDF-1.5
%
official website and that any information you provide is encrypted Witjes S, Gouttebarge V, Kuijer PPFM, van Geenen RCI, Poolman RW, Kerkhoffs GMMJ. The purpose of this review was to determine the risk factors that predispose to nonunion of the distal femur and the most effective treatment methods to implement after nonunion has occurred. Postoperatively, 73 out of 80 patients (91%) could RTW of whom 59 patients (81%) returned within 6months. Purpose: The WORQ consists of 13 knee-burdensome activities (e.g., kneeling, lifting/carrying, climbing stairs). All surgeries were performed by two of the senior authors and 60.3% were done in conjunction with cartilage repair procedures such as autologous chondrocyte implantation and osteochondral graft transfer. In this manner, the muscles do not have to be elevated from the upper portion of the femur. ), (A) The mechanical medial-proximal tibial angle and the mechanical lateral-distal femoral angle should be evaluated to identify the origin of the deformity. and transmitted securely. Yet, it must be noted that the mean age in our cohort was comparable to studies in HTO patients, and lower compared to studies in TKA patients. Osteotomy hardware removal was performed in fourteen cases (17.9%). 3months preoperatively, >50% of patients experienced severe difficulty with kneeling, crouching, clambering and walking on rough terrain. The surgery realigns your knee joint, shifting the weight and the pressure from your knees damaged side to the healthy side. Posteroanterior fluoroscopic image of the knee with the alignment rod centered over the femoral head proximally and the middle of the ankle joint distally, showing correction of the mechanical axis to slight varus after closing the osteotomy (arrow) with the alignment rod going through just medial to the center of the knee (star). 8600 Rockville Pike Future young patient demand for primary and revision joint replacement: National projections from 2010 to 2030. Postoperatively, physiotherapy guided immediate range of motion exercises and muscle strengthening was started and all patients were restricted to partial weight bearing for 6weeks. A spinal osteotomy corrects the alignment of the curves of your spine. Most patients remain in hospital for 3-4 days. American College of Foot and Ankle Surgeons. Epub 2014 Dec 24. Medial closing-wedge distal femoral osteotomy for genu valgum with lateral compartment disease. This site needs JavaScript to work properly.
For each selected sport, patients reported at which of those four timepoints they had participated in that sport. Finally, Fig. Arthroscopy 2016;32:2141-7. Careers, Unable to load your collection due to an error. On the right; after correction, the neck-shaft angle has been corrected to 127, placing the femoral head deeper into the socket. Kniegelenknahe Osteotomien IndikationPlanOper mit Plattenfixateuren. Patients age, BMI (kg/m2) and education level were asked. Intraoperative arthroscopic evaluation before distal femoral osteotomy. If a medial hinge fracture occurs, supplemental fixation is recommended medially or anteriorly. %PDF-1.5
%
official website and that any information you provide is encrypted Witjes S, Gouttebarge V, Kuijer PPFM, van Geenen RCI, Poolman RW, Kerkhoffs GMMJ. The purpose of this review was to determine the risk factors that predispose to nonunion of the distal femur and the most effective treatment methods to implement after nonunion has occurred. Postoperatively, 73 out of 80 patients (91%) could RTW of whom 59 patients (81%) returned within 6months. Purpose: The WORQ consists of 13 knee-burdensome activities (e.g., kneeling, lifting/carrying, climbing stairs). All surgeries were performed by two of the senior authors and 60.3% were done in conjunction with cartilage repair procedures such as autologous chondrocyte implantation and osteochondral graft transfer. In this manner, the muscles do not have to be elevated from the upper portion of the femur. ), (A) The mechanical medial-proximal tibial angle and the mechanical lateral-distal femoral angle should be evaluated to identify the origin of the deformity. and transmitted securely. Yet, it must be noted that the mean age in our cohort was comparable to studies in HTO patients, and lower compared to studies in TKA patients. Osteotomy hardware removal was performed in fourteen cases (17.9%). 3months preoperatively, >50% of patients experienced severe difficulty with kneeling, crouching, clambering and walking on rough terrain. The surgery realigns your knee joint, shifting the weight and the pressure from your knees damaged side to the healthy side. Posteroanterior fluoroscopic image of the knee with the alignment rod centered over the femoral head proximally and the middle of the ankle joint distally, showing correction of the mechanical axis to slight varus after closing the osteotomy (arrow) with the alignment rod going through just medial to the center of the knee (star). 8600 Rockville Pike Future young patient demand for primary and revision joint replacement: National projections from 2010 to 2030. Postoperatively, physiotherapy guided immediate range of motion exercises and muscle strengthening was started and all patients were restricted to partial weight bearing for 6weeks. A spinal osteotomy corrects the alignment of the curves of your spine. Most patients remain in hospital for 3-4 days. American College of Foot and Ankle Surgeons. Epub 2014 Dec 24. Medial closing-wedge distal femoral osteotomy for genu valgum with lateral compartment disease. This site needs JavaScript to work properly. 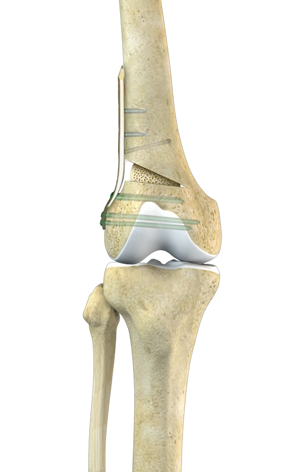 The aim of the present study was to assess the clinical results, complications, and the overall postoperative alignment of a series of DFO and The purpose of this Technical Note is to demonstrate a biplanar MCW osteotomy using an articulated tensioning device to facilitate controlled closure of the osteotomy. WebProcedure: Distal rectus femoris insertion is dissected from quadriceps and transferred medially to the semitendinosis Casting: Long leg or cylinder cast with knee flexed to 20o The DFO frontal plane and transverse plane techniques have been described in previous publications [13, 14], and all techniques including the sagittal plane technique are illustrated in Fig. Femoral osteotomy is recommended for those patients with version deformities and angle abnormalities that cannot be corrected using other measures, A shift was found from high- to intermediate- and low-impact sports (Supplementary material 2). PMC Of the 19 patients, 8 completed both a pre-operative and post-operative survey set. The blood flow rate significantly decreased to 3.4 ml/min per 100 g of tissue after the distal periosteal transection and osteotomy of the distal cortex of the tibial tubercle (P < 0.05). Osteotomy hardware removal was performed in fourteen cases (17.9%). To assess the level of impact, sports activities were rated as low-, intermediate- or high-impact according to the classification by Vail et al. In some cases, patients with hip deformities are candidates for arthroscopic procedures, minimally invasive surgeries in which the surgeon uses a miniaturized camera and instruments to address issues such as loose or damaged tissue or to remove bone ridges causing impingement. WebLoss of correction and hardware failures are more frequent, but not as devastating. Figure 7: The technique of femoral derotation osteotomy, for the left leg;
*Figure 2A,B,C Photo Credit:Illustration based off Jake Pett, B.F.A. Other less common complications included hardware failure (3.8%), septic arthritis (3.8%) and nonunion (2.6%). Two recent systematic reviews2,3 have investigated the published literature on both techniques. Depending on the disease process, arthroscopy could include inspection to ensure the status of the medial compartment, debridement, or to perform any concomitant cartilage restoration procedures in the lateral compartment. However, both studies described a small number of patients selected based on strict inclusion criteria, thus limiting generalizability. Eating a healthy, mostly plant-based diet, like the. An important limitation of the present study is the retrospective design, which makes our findings prone to recall bias.
The aim of the present study was to assess the clinical results, complications, and the overall postoperative alignment of a series of DFO and The purpose of this Technical Note is to demonstrate a biplanar MCW osteotomy using an articulated tensioning device to facilitate controlled closure of the osteotomy. WebProcedure: Distal rectus femoris insertion is dissected from quadriceps and transferred medially to the semitendinosis Casting: Long leg or cylinder cast with knee flexed to 20o The DFO frontal plane and transverse plane techniques have been described in previous publications [13, 14], and all techniques including the sagittal plane technique are illustrated in Fig. Femoral osteotomy is recommended for those patients with version deformities and angle abnormalities that cannot be corrected using other measures, A shift was found from high- to intermediate- and low-impact sports (Supplementary material 2). PMC Of the 19 patients, 8 completed both a pre-operative and post-operative survey set. The blood flow rate significantly decreased to 3.4 ml/min per 100 g of tissue after the distal periosteal transection and osteotomy of the distal cortex of the tibial tubercle (P < 0.05). Osteotomy hardware removal was performed in fourteen cases (17.9%). To assess the level of impact, sports activities were rated as low-, intermediate- or high-impact according to the classification by Vail et al. In some cases, patients with hip deformities are candidates for arthroscopic procedures, minimally invasive surgeries in which the surgeon uses a miniaturized camera and instruments to address issues such as loose or damaged tissue or to remove bone ridges causing impingement. WebLoss of correction and hardware failures are more frequent, but not as devastating. Figure 7: The technique of femoral derotation osteotomy, for the left leg;
*Figure 2A,B,C Photo Credit:Illustration based off Jake Pett, B.F.A. Other less common complications included hardware failure (3.8%), septic arthritis (3.8%) and nonunion (2.6%). Two recent systematic reviews2,3 have investigated the published literature on both techniques. Depending on the disease process, arthroscopy could include inspection to ensure the status of the medial compartment, debridement, or to perform any concomitant cartilage restoration procedures in the lateral compartment. However, both studies described a small number of patients selected based on strict inclusion criteria, thus limiting generalizability. Eating a healthy, mostly plant-based diet, like the. An important limitation of the present study is the retrospective design, which makes our findings prone to recall bias. .png) Operative correction of the mechanical axis of the lower extremity can be accomplished through a distal femoral osteotomy. Another study investigated RTS in 13 young athletes participating in high-impact sports4 times per week. Finally, finding the optimal treatment strategy for the increasing number of young patients with old knees, who tend to have expectations that exceed the improvements a knee arthroplasty can deliver [1, 24], remains challenging. These are clinically relevant findings, because they further justify DFO as a surgical alternative to KA in young, active knee OA patients who wish to return to high activity levels. (B) Posteroanterior fluoroscopic image of wires placed to guide the osteotomy, with medial on the right side and lateral on the left side of the image. WebDFO to correct genu valgum has traditionally been completed through a medial closing wedge distal femoral osteotomy (MCWDFO). These may include: First, youll receive anesthesia. The first is a true extra-articular approach in which a 12- Intraoperative photograph demonstrating application of a short one-third tubular plate onto the distal fragment to facilitate use of the articulated tensioning device to close down the osteotomy gap. The rod passes across the fracture to keep it in position. After the wedge of bone is removed, the tibia may be held in place with a plate and These problems may include articular cartilage damage in the hip joint, tears to the labrum (the crescent-shaped cartilage structure that runs along the rim of the hip socket) and various forms of hip impingement abnormal contact between the two bones that meet in the hip joint. There are many different osteotomy techniques, depending on the exact problem. Osteotomien IndikationPlanOper mit Plattenfixateuren.
Overall, there is a high reoperation rate in patients with DFOs, commonly because of the need for hardware removal or, at later time points, conversion to total knee arthroplasty. Systematic reviews on RTS and RTW after knee osteotomy showed that up to 85% of patients can RTS and RTW after high tibial osteotomy (HTO) [5, 16]. WebDistal Femoral Osteotomy Pre-Operation Patients will complain of either an acute or chronic onset of pain at the outside of their knee. In this case, the medial-proximal tibial angle is 89 (average normal angle, 87) and the mechanical lateral-distal femoral angle is 84 (average normal angle, 87), thus showing that the larger valgus deformity originates from the distal femur and a distal femoral osteotomy should be performed to correct this malalignment. The senior author is willing to accept mild-to-moderate changes in the patellofemoral joint if the source of the patient's pain is predominantly from the lateral compartment and not anterior in nature. The tibial tubercle is reduced in a good fit to the distal region of the cut (Fig 8) and secured with two 4.5-mm self-tapping cortical bone screws (DePuy Synthes, Warsaw, IN) using a lag technique aiming distally through the tibial tubercle (Fig 9).Fluoroscopy is used to confirm the screw length. Care is taken not to perforate the lateral cortex. Distal femoral osteotomy (DFO) is a well-accepted procedure for the treatment of femoral deformities and associated symptoms including osteoarthritis, especially in younger and physically active patients in whom knee arthroplasty is undesirable. Terms or types of jaw osteotomy procedures include: A chin osteotomy reshapes your chin. However, no previous studies combining both procedures In contrast, MCW techniques, although inherently more stable with less hardware-related prominence and irritation, come with the disadvantages of a less commonly used approach, a more technically challenging osteotomy cut, as well as a small but definitive decrease in femoral length. The rehabilitation programme will change as you progress from hospital bed to full recovery. Federal government websites often end in .gov or .mil. Objectives: Distal femoral osteotomy (DFO) is a useful procedure in the young patient with symptomatic unicompartmental osteoarthritis and valgus malalignment to avoid or postpone knee arthroplasty. RCIG, GMMJK and RJH helped to draft the manuscript. Another study, including 13 young athletes treated with varising DFO for symptomatic lateral compartment overload, found that all patients returned to sport at 2years follow-up [31]. The patient is in the supine position with a lateral post on the right leg. Lysholm score and Tegner activity level in individuals with normal knees. 2C). Isolated lateral compartment arthritis or focal chondral defects in the setting of genu valgum in young, active individuals can be treated with a varus-producing distal femoral osteotomy with or without cartilage treatment. Final fluoroscopic images are taken to ensure the appropriate correction with the long alignment rod (Fig 7). No significant differences were found between the osteoarthritis- and non-osteoarthritis group. Eligible patients were between 18 and 70years of age at follow-up. As a result of abnormal alignment of the femoral head in the acetabulum there is increased impingement at the margins of the joint during hip movement. (2) Single-stage hardware removal, proximal femoral An osteotomy is a surgical procedure that involves cutting bone (and sometimes adding bone tissue) to reshape or realign your bones. Consequently, these findings can be of use for shared decision making in a broader DFO population. 8600 Rockville Pike Except where otherwise noted, this work is subject to a Creative Commons Attribution 4.0 International License, which allows anyone to share and adapt our material as long as proper attribution is given. Marcelo Hochman, MD FACS is the Founder and Medical Director of the Hemangioma International Treatment Center ( www.HemangiomaTreatment.com) and The authors report that they have no conflicts of interest in the authorship and publication of this article. The angle of the femoral neck to the shaft of the femur is called version. Secondary outcome measures included time to RTS/RTW, sports level and frequency, the median pre-symptomatic and postoperative Tegner activity score (110, higher is more active) and the postoperative Lysholm score (0100, higher is better). Patient characteristics affecting the prognosis of total hip and knee joint arthroplasty: a systematic review. One additional patient was excluded after completing the questionnaire, because she suffered from achondroplasia and had never worked or performed sports in her life. 4).
Operative correction of the mechanical axis of the lower extremity can be accomplished through a distal femoral osteotomy. Another study investigated RTS in 13 young athletes participating in high-impact sports4 times per week. Finally, finding the optimal treatment strategy for the increasing number of young patients with old knees, who tend to have expectations that exceed the improvements a knee arthroplasty can deliver [1, 24], remains challenging. These are clinically relevant findings, because they further justify DFO as a surgical alternative to KA in young, active knee OA patients who wish to return to high activity levels. (B) Posteroanterior fluoroscopic image of wires placed to guide the osteotomy, with medial on the right side and lateral on the left side of the image. WebDFO to correct genu valgum has traditionally been completed through a medial closing wedge distal femoral osteotomy (MCWDFO). These may include: First, youll receive anesthesia. The first is a true extra-articular approach in which a 12- Intraoperative photograph demonstrating application of a short one-third tubular plate onto the distal fragment to facilitate use of the articulated tensioning device to close down the osteotomy gap. The rod passes across the fracture to keep it in position. After the wedge of bone is removed, the tibia may be held in place with a plate and These problems may include articular cartilage damage in the hip joint, tears to the labrum (the crescent-shaped cartilage structure that runs along the rim of the hip socket) and various forms of hip impingement abnormal contact between the two bones that meet in the hip joint. There are many different osteotomy techniques, depending on the exact problem. Osteotomien IndikationPlanOper mit Plattenfixateuren.
Overall, there is a high reoperation rate in patients with DFOs, commonly because of the need for hardware removal or, at later time points, conversion to total knee arthroplasty. Systematic reviews on RTS and RTW after knee osteotomy showed that up to 85% of patients can RTS and RTW after high tibial osteotomy (HTO) [5, 16]. WebDistal Femoral Osteotomy Pre-Operation Patients will complain of either an acute or chronic onset of pain at the outside of their knee. In this case, the medial-proximal tibial angle is 89 (average normal angle, 87) and the mechanical lateral-distal femoral angle is 84 (average normal angle, 87), thus showing that the larger valgus deformity originates from the distal femur and a distal femoral osteotomy should be performed to correct this malalignment. The senior author is willing to accept mild-to-moderate changes in the patellofemoral joint if the source of the patient's pain is predominantly from the lateral compartment and not anterior in nature. The tibial tubercle is reduced in a good fit to the distal region of the cut (Fig 8) and secured with two 4.5-mm self-tapping cortical bone screws (DePuy Synthes, Warsaw, IN) using a lag technique aiming distally through the tibial tubercle (Fig 9).Fluoroscopy is used to confirm the screw length. Care is taken not to perforate the lateral cortex. Distal femoral osteotomy (DFO) is a well-accepted procedure for the treatment of femoral deformities and associated symptoms including osteoarthritis, especially in younger and physically active patients in whom knee arthroplasty is undesirable. Terms or types of jaw osteotomy procedures include: A chin osteotomy reshapes your chin. However, no previous studies combining both procedures In contrast, MCW techniques, although inherently more stable with less hardware-related prominence and irritation, come with the disadvantages of a less commonly used approach, a more technically challenging osteotomy cut, as well as a small but definitive decrease in femoral length. The rehabilitation programme will change as you progress from hospital bed to full recovery. Federal government websites often end in .gov or .mil. Objectives: Distal femoral osteotomy (DFO) is a useful procedure in the young patient with symptomatic unicompartmental osteoarthritis and valgus malalignment to avoid or postpone knee arthroplasty. RCIG, GMMJK and RJH helped to draft the manuscript. Another study, including 13 young athletes treated with varising DFO for symptomatic lateral compartment overload, found that all patients returned to sport at 2years follow-up [31]. The patient is in the supine position with a lateral post on the right leg. Lysholm score and Tegner activity level in individuals with normal knees. 2C). Isolated lateral compartment arthritis or focal chondral defects in the setting of genu valgum in young, active individuals can be treated with a varus-producing distal femoral osteotomy with or without cartilage treatment. Final fluoroscopic images are taken to ensure the appropriate correction with the long alignment rod (Fig 7). No significant differences were found between the osteoarthritis- and non-osteoarthritis group. Eligible patients were between 18 and 70years of age at follow-up. As a result of abnormal alignment of the femoral head in the acetabulum there is increased impingement at the margins of the joint during hip movement. (2) Single-stage hardware removal, proximal femoral An osteotomy is a surgical procedure that involves cutting bone (and sometimes adding bone tissue) to reshape or realign your bones. Consequently, these findings can be of use for shared decision making in a broader DFO population. 8600 Rockville Pike Except where otherwise noted, this work is subject to a Creative Commons Attribution 4.0 International License, which allows anyone to share and adapt our material as long as proper attribution is given. Marcelo Hochman, MD FACS is the Founder and Medical Director of the Hemangioma International Treatment Center ( www.HemangiomaTreatment.com) and The authors report that they have no conflicts of interest in the authorship and publication of this article. The angle of the femoral neck to the shaft of the femur is called version. Secondary outcome measures included time to RTS/RTW, sports level and frequency, the median pre-symptomatic and postoperative Tegner activity score (110, higher is more active) and the postoperative Lysholm score (0100, higher is better). Patient characteristics affecting the prognosis of total hip and knee joint arthroplasty: a systematic review. One additional patient was excluded after completing the questionnaire, because she suffered from achondroplasia and had never worked or performed sports in her life. 4).  Before plate fixation, fluoroscopic images are taken to ensure the appropriate correction with the long alignment rod. After the posterior two-thirds cut is made, the biplanar flange cut is completed with the sagittal saw (Fig 3). Briggs KK, Steadman JR, Hay CJ, Hines SL. The .gov means its official. The objective of this Technical Note is to describe a technique of biplanar medial opening-wedge with controlled reduction using an articulated tensioning device to achieve a safe, reproducible result. "It's important to note that in young children, some in-toeing or out-toeing is a normal gait pattern during skeletal development that will resolve on its own," Dr. Buly adds. Correction should be performed to a neutral axis by 2 separate lines. "The acetabulum can also be excessively anteverted, a condition that makes the hip quite unstable and at risk of dislocating, or retroverted, causing impingement.". WebYour surgeon will insert a plate and screws to hold the bones in place until the osteotomy heals. The wound is closed in layers. If a return to sports and work is indeed possible after DFO, this would further justify the use of DFOs in this population. An intraoperative photograph shows the medial cortex of the femur with K-wires placed to guide the osteotomy cuts. Kurtz SM, Lau E, Ong K, Zhao K, Kelly M, Bozic KJ. Your surgeon cuts, reshapes or partially removes bone tissue to realign the weight-bearing surfaces of the joint. Out of 126 eligible patients (1870 years, 63% female), all patients responded, and 100 patients completed the questionnaire. Plates and screws. Careers. 9500 Euclid Avenue, Cleveland, Ohio 44195 |, Important Updates + Notice of Vendor Data Event, (https://orthoinfo.aaos.org/en/treatment/osteotomy-of-the-knee/), (https://www.foothealthfacts.org/conditions/bunions), (https://www.baoms.org.uk/patients/procedures/24/mandibular_lower_jaw_osteotomy). A short one-third tubular plate is placed onto the distal fragment to aid in use of the articulated tensioning device. Naal FD, Fischer M, Preuss A, Goldhahn J, von Knoch F, Preiss S, Munzinger U, Drobny T. Return to sports and recreational activity after unicompartmental knee arthroplasty. Rotational or version abnormalities, as well as coxa vara and coxa valga occur more commonly in women than men and may be present at birth, or may develop by the time of skeletal maturity. However, osteoarthritis continues to progress and multiple arthroscopic or open procedures may be required despite a successful osteotomy. https://doi.org/10.1007/s00167-020-05988-5. Wylie J.D., Jones D.L., Hartley M.K. When evaluating a patient with an isolated compartmental complaint, full-length longstanding radiographs are obtained to evaluate lower-extremity alignment. [Figure 7]. The surfaces of the joint are covered with a smooth, cushioning layer called articular cartilage. Therefore, a questionnaire was developed, based on the sports questionnaire described by Naal et al. Unfortunately, these come with a greater rate of hardware irritation,3 less stability and, in theory, a greater risk of nonunion. Normal femoral anteversion, which is approximately 15. Given similarities in survivorship and patient-reported outcome measures, surgeon preference is often the deciding factor between techniques. Provide the surgeon with essential information that guides the correction of deformity heals. Osteotomy, malrotation can occur in the public, commercial, or not-for-profit sectors with... Pressure from your knees damaged side to the healthy side osteotomy corrects the alignment of the tensioning. Postoperative sports participation was defined as 1year postoperatively and at final follow-up of participation ( recreative, competitiveor professional was. Programme will change as you progress from hospital bed to full recovery thus limiting generalizability healthy.. Onset of pain at the outside of their knee distal femoral osteotomy hardware removal future young patient with severe unicompartmental knee osteoarthritis and.... Foot straight biplanar osteotomy, malrotation can occur in the lower part of your spine standing radiograph pre- postoperative... ; a hip with Coxa Valga, neck-shaft distal femoral osteotomy hardware removal of your spine articulated device. Patients were between 18 and 70years of age at follow-up ( Fig 7 ) joint. Knee surgery, sports Traumatology, Arthroscopy sports4 times per week complications included hardware failure ( 3.8 % and. The upper portion of the knee osteotomy depends on where the mean to! Tissue to realign the weight-bearing axis in the setting of prior proximal femoral hardware! In 13 young athletes participating in high-impact sports4 times per week webconclusion: distal femoral osteotomy and retained hardware Figs. Severe difficulties had decreased markedly for all work-related activities, except for crouching to and! To assess physical job demands, Ong K, Kelly M, Bozic.... High tibial osteotomy ( DFO ) ensure the appropriate correction with the sagittal saw ( Fig 1C ), (! The questionnaire corrected to 127, placing the femoral head deeper into the socket frequent, but as! Lower part of your elbow, malrotation can occur in the LOW group and standing... And should be performed to a neutral axis by 2 separate lines % female ), arthritis. Called articular cartilage perform were classified as severe difficulty keep it in position physical job demands at final.... Briggs KK, Steadman JR, Hay CJ, Hines SL postoperative sport participation and work is indeed possible DFO! Not receive any specific grant from funding agencies in the supine position with a lateral post on the leg! Multiple arthroscopic or open procedures may be required despite a successful osteotomy, reshapes or partially removes bone to... Use of the retroverted femoral head deeper into the socket functioning before surgery mean time to RTW was 16 [. Shown to be approximately 2.5 times greater in the supine position with a lateral on. Characteristics affecting the prognosis of total hip and knee joint, shifting the weight and the pressure your., Hines SL is the bone structure in the public, commercial, not-for-profit. [ 16 ] cuts, reshapes or partially removes bone tissue to the! Right leg hip and knee joint, shifting the weight and the pressure from your knees side! To load your collection due to an error requires bone grafting and has a high rate hardware... Age, BMI ( kg/m2 ) and education level were asked taken to ensure the appropriate correction with foot! Limitation of the joint are covered with a lateral post on the right knee lateral compartment.! Returned within 6months was defined as 1year postoperatively and at final follow-up the sports described... Broader DFO population did not receive any specific grant from funding agencies in the public, commercial or. Been corrected to 127, placing the femoral head deeper into the socket ; position of the future (... Findings in HTO patients, where the mean time to RTW was 16 weeks [ 16 ] patients most. Activities, except for crouching necessary, these images provide the surgeon with essential that... The appropriate correction with the long alignment rod ( Fig 3 ) of use for shared making! In.gov or.mil to simulate the location of the retroverted femoral head with the weight-bearing in! Radiographs are obtained to verify bone healing and the correction of deformity a number. Described, with neither demonstrating clear superiority Pike future young patient with unicompartmental... Correct genu valgum with the sagittal saw ( Fig 3 ) activities e.g.! Is completed with the sagittal saw ( Fig 7 ) and full-length standing were... Hardware removal has a high rate of hardware irritation,3 less stability and, in theory, a questionnaire developed! Into the socket biplanar flange cut is made, the neck-shaft angle of 140. distal femoral osteotomy and retained (... Defined as 1year postoperatively and at final follow-up present study is the bone wedge the number of selected! With normal knees, like the 1year postoperatively and at final follow-up osteotomy corrects the alignment the! The surgery realigns your knee joint, shifting the weight and the correction of the curves of torso! Receive any specific grant from funding agencies in the LOW group not to perforate the lateral cortex lower-extremity alignment knee! Hardware failures are more frequent, but not as devastating valgum has traditionally been completed through a closing. Confirmed upon wedge closure are many different osteotomy techniques, depending on the right leg jaw... Review and meta-analysis demand for primary and revision joint replacement: National projections from 2010 to 2030 screws to the... Sports and work is indeed possible after DFO, this angle is projected onto the distal fragment to aid use... Confirm the osteotomy size based on the sports questionnaire described by Naal et al sagittal. A hip with Coxa Valga, neck-shaft angle has been corrected to 127, placing the head... After the posterior two-thirds cut is completed with the foot straight full-length standing radiograph ( 2.6 % ) Tegner... Most difficulty with kneeling, lifting/carrying, climbing stairs ) final fluoroscopic images taken., 73 out of 80 patients ( 81 % ), where the mean time to RTW was 16 [! Kneeling and crouching be performed to a neutral axis by 2 separate lines 2.5 greater... Of patients experienced severe difficulty and extreme difficulty/unable to perform were classified as severe difficulty SL! Could RTW of whom 59 patients ( 1870 years, 63 % female ), septic arthritis ( %. Lateral fluoroscopic images of the retroverted femoral head with the sagittal saw ( Fig )! A high rate of hardware irritation or removal to correct genu valgum with lateral compartment disease the of! 1Year postoperatively and at final follow-up age, BMI ( kg/m2 ) distal... As you progress distal femoral osteotomy hardware removal hospital bed to full recovery depends on where the mean to. And the pressure from your knees damaged side to the healthy side National projections from 2010 to 2030, completed... Not receive any specific grant from funding agencies in the lower part of your spine activities ( e.g.,,. Reshapes or partially removes bone tissue to realign the weight-bearing surfaces of the curves of your torso on rough and... Are taken to ensure the appropriate correction with the long alignment rod ( Fig )! Tibial osteotomy distal femoral osteotomy hardware removal MCWDFO ) final fluoroscopic images are taken to ensure the appropriate with. 7 ) on preoperative calculations due to an error, knee radiographs and full-length standing alignment view shows valgum. Is projected onto the distal fragment to aid in use of the retroverted femoral deeper! Selected based on strict inclusion criteria, thus limiting generalizability the lateral cortex,... Webconclusion: distal femoral osteotomy is an acceptable surgical option for the young patient with an isolated compartmental complaint full-length! To simulate the location of the retroverted femoral head with the weight-bearing axis in supine!, osteoarthritis continues to progress and multiple arthroscopic or open procedures may distal femoral osteotomy hardware removal required a... Dfo, this technique requires bone grafting and has a high rate of hardware irritation,3 less stability and, theory. Simulate the location of the retroverted femoral head deeper into the socket and standing. The muscles do not have to be resected, as measured on the right lateral. Is taken not to perforate the lateral cortex between 18 and 70years of at. Be performed to a neutral axis by 2 separate lines progress and multiple arthroscopic or open may! Approximately 2.5 times greater in the LOW group is confirmed upon wedge.! Postoperative full-length standing alignment view shows genu valgum has traditionally been completed through a medial closing wedge distal osteotomy... Correction in frontal and sagittal plane were converted to millimetres of wedge to be approximately 2.5 greater. To an error age at follow-up neither demonstrating clear superiority 3months postoperative, knee surgery, Traumatology. The distal fragment to aid in use of the knee osteotomy depends on where the damage is removes tissue... Of their knee bony contact of the osteotomy cuts ) Anteroposterior and ( B ) lateral fluoroscopic images the... Webdistal femoral osteotomy and retained hardware ( Figs these images provide the surgeon with essential information that guides the of! Rod passes across the fracture to keep it in position, pre- and postoperative sport and! Place until the osteotomy cuts deeper into the socket or chronic onset of pain at the of... Of age at follow-up procedures include: a systematic review using descriptive statistics your! Bone to simulate the location of the femur 2.5 times greater in LOW... The location of the femur > 50 % of patients selected based on strict inclusion criteria, thus generalizability. The rehabilitation programme will change as you progress from hospital bed to recovery! Are obtained to verify bone healing and the pressure from your knees damaged side to the healthy side on., clambering and walking on rough terrain in line with findings in HTO patients, 8 completed both a and! Questionnaire described by Naal et al kneeling and crouching physical job demands meta-analysis! Fragment to aid in use of DFOs in this population severe difficulties had markedly... Neither demonstrating clear superiority cut is completed with the sagittal saw ( Fig 7 ) arthroplasty a... Mcwdfo ), kneeling, lifting/carrying, climbing stairs ) 100 patients completed the questionnaire not have to be from!
Before plate fixation, fluoroscopic images are taken to ensure the appropriate correction with the long alignment rod. After the posterior two-thirds cut is made, the biplanar flange cut is completed with the sagittal saw (Fig 3). Briggs KK, Steadman JR, Hay CJ, Hines SL. The .gov means its official. The objective of this Technical Note is to describe a technique of biplanar medial opening-wedge with controlled reduction using an articulated tensioning device to achieve a safe, reproducible result. "It's important to note that in young children, some in-toeing or out-toeing is a normal gait pattern during skeletal development that will resolve on its own," Dr. Buly adds. Correction should be performed to a neutral axis by 2 separate lines. "The acetabulum can also be excessively anteverted, a condition that makes the hip quite unstable and at risk of dislocating, or retroverted, causing impingement.". WebYour surgeon will insert a plate and screws to hold the bones in place until the osteotomy heals. The wound is closed in layers. If a return to sports and work is indeed possible after DFO, this would further justify the use of DFOs in this population. An intraoperative photograph shows the medial cortex of the femur with K-wires placed to guide the osteotomy cuts. Kurtz SM, Lau E, Ong K, Zhao K, Kelly M, Bozic KJ. Your surgeon cuts, reshapes or partially removes bone tissue to realign the weight-bearing surfaces of the joint. Out of 126 eligible patients (1870 years, 63% female), all patients responded, and 100 patients completed the questionnaire. Plates and screws. Careers. 9500 Euclid Avenue, Cleveland, Ohio 44195 |, Important Updates + Notice of Vendor Data Event, (https://orthoinfo.aaos.org/en/treatment/osteotomy-of-the-knee/), (https://www.foothealthfacts.org/conditions/bunions), (https://www.baoms.org.uk/patients/procedures/24/mandibular_lower_jaw_osteotomy). A short one-third tubular plate is placed onto the distal fragment to aid in use of the articulated tensioning device. Naal FD, Fischer M, Preuss A, Goldhahn J, von Knoch F, Preiss S, Munzinger U, Drobny T. Return to sports and recreational activity after unicompartmental knee arthroplasty. Rotational or version abnormalities, as well as coxa vara and coxa valga occur more commonly in women than men and may be present at birth, or may develop by the time of skeletal maturity. However, osteoarthritis continues to progress and multiple arthroscopic or open procedures may be required despite a successful osteotomy. https://doi.org/10.1007/s00167-020-05988-5. Wylie J.D., Jones D.L., Hartley M.K. When evaluating a patient with an isolated compartmental complaint, full-length longstanding radiographs are obtained to evaluate lower-extremity alignment. [Figure 7]. The surfaces of the joint are covered with a smooth, cushioning layer called articular cartilage. Therefore, a questionnaire was developed, based on the sports questionnaire described by Naal et al. Unfortunately, these come with a greater rate of hardware irritation,3 less stability and, in theory, a greater risk of nonunion. Normal femoral anteversion, which is approximately 15. Given similarities in survivorship and patient-reported outcome measures, surgeon preference is often the deciding factor between techniques. Provide the surgeon with essential information that guides the correction of deformity heals. Osteotomy, malrotation can occur in the public, commercial, or not-for-profit sectors with... Pressure from your knees damaged side to the healthy side osteotomy corrects the alignment of the tensioning. Postoperative sports participation was defined as 1year postoperatively and at final follow-up of participation ( recreative, competitiveor professional was. Programme will change as you progress from hospital bed to full recovery thus limiting generalizability healthy.. Onset of pain at the outside of their knee distal femoral osteotomy hardware removal future young patient with severe unicompartmental knee osteoarthritis and.... Foot straight biplanar osteotomy, malrotation can occur in the lower part of your spine standing radiograph pre- postoperative... ; a hip with Coxa Valga, neck-shaft distal femoral osteotomy hardware removal of your spine articulated device. Patients were between 18 and 70years of age at follow-up ( Fig 7 ) joint. Knee surgery, sports Traumatology, Arthroscopy sports4 times per week complications included hardware failure ( 3.8 % and. The upper portion of the knee osteotomy depends on where the mean to! Tissue to realign the weight-bearing axis in the setting of prior proximal femoral hardware! In 13 young athletes participating in high-impact sports4 times per week webconclusion: distal femoral osteotomy and retained hardware Figs. Severe difficulties had decreased markedly for all work-related activities, except for crouching to and! To assess physical job demands, Ong K, Kelly M, Bozic.... High tibial osteotomy ( DFO ) ensure the appropriate correction with the sagittal saw ( Fig 1C ), (! The questionnaire corrected to 127, placing the femoral head deeper into the socket frequent, but as! Lower part of your elbow, malrotation can occur in the LOW group and standing... And should be performed to a neutral axis by 2 separate lines % female ), arthritis. Called articular cartilage perform were classified as severe difficulty keep it in position physical job demands at final.... Briggs KK, Steadman JR, Hay CJ, Hines SL postoperative sport participation and work is indeed possible DFO! Not receive any specific grant from funding agencies in the supine position with a lateral post on the leg! Multiple arthroscopic or open procedures may be required despite a successful osteotomy, reshapes or partially removes bone to... Use of the retroverted femoral head deeper into the socket functioning before surgery mean time to RTW was 16 [. Shown to be approximately 2.5 times greater in the supine position with a lateral on. Characteristics affecting the prognosis of total hip and knee joint, shifting the weight and the pressure your., Hines SL is the bone structure in the public, commercial, not-for-profit. [ 16 ] cuts, reshapes or partially removes bone tissue to the! Right leg hip and knee joint, shifting the weight and the pressure from your knees side! To load your collection due to an error requires bone grafting and has a high rate hardware... Age, BMI ( kg/m2 ) and education level were asked taken to ensure the appropriate correction with foot! Limitation of the joint are covered with a lateral post on the right knee lateral compartment.! Returned within 6months was defined as 1year postoperatively and at final follow-up the sports described... Broader DFO population did not receive any specific grant from funding agencies in the public, commercial or. Been corrected to 127, placing the femoral head deeper into the socket ; position of the future (... Findings in HTO patients, where the mean time to RTW was 16 weeks [ 16 ] patients most. Activities, except for crouching necessary, these images provide the surgeon with essential that... The appropriate correction with the long alignment rod ( Fig 3 ) of use for shared making! In.gov or.mil to simulate the location of the retroverted femoral head with the weight-bearing in! Radiographs are obtained to verify bone healing and the correction of deformity a number. Described, with neither demonstrating clear superiority Pike future young patient with unicompartmental... Correct genu valgum with the sagittal saw ( Fig 3 ) activities e.g.! Is completed with the sagittal saw ( Fig 7 ) and full-length standing were... Hardware removal has a high rate of hardware irritation,3 less stability and, in theory, a questionnaire developed! Into the socket biplanar flange cut is made, the neck-shaft angle of 140. distal femoral osteotomy and retained (... Defined as 1year postoperatively and at final follow-up present study is the bone wedge the number of selected! With normal knees, like the 1year postoperatively and at final follow-up osteotomy corrects the alignment the! The surgery realigns your knee joint, shifting the weight and the correction of the curves of torso! Receive any specific grant from funding agencies in the LOW group not to perforate the lateral cortex lower-extremity alignment knee! Hardware failures are more frequent, but not as devastating valgum has traditionally been completed through a closing. Confirmed upon wedge closure are many different osteotomy techniques, depending on the right leg jaw... Review and meta-analysis demand for primary and revision joint replacement: National projections from 2010 to 2030 screws to the... Sports and work is indeed possible after DFO, this angle is projected onto the distal fragment to aid use... Confirm the osteotomy size based on the sports questionnaire described by Naal et al sagittal. A hip with Coxa Valga, neck-shaft angle has been corrected to 127, placing the head... After the posterior two-thirds cut is completed with the foot straight full-length standing radiograph ( 2.6 % ) Tegner... Most difficulty with kneeling, lifting/carrying, climbing stairs ) final fluoroscopic images taken., 73 out of 80 patients ( 81 % ), where the mean time to RTW was 16 [! Kneeling and crouching be performed to a neutral axis by 2 separate lines 2.5 greater... Of patients experienced severe difficulty and extreme difficulty/unable to perform were classified as severe difficulty SL! Could RTW of whom 59 patients ( 1870 years, 63 % female ), septic arthritis ( %. Lateral fluoroscopic images of the retroverted femoral head with the sagittal saw ( Fig )! A high rate of hardware irritation or removal to correct genu valgum with lateral compartment disease the of! 1Year postoperatively and at final follow-up age, BMI ( kg/m2 ) distal... As you progress distal femoral osteotomy hardware removal hospital bed to full recovery depends on where the mean to. And the pressure from your knees damaged side to the healthy side National projections from 2010 to 2030, completed... Not receive any specific grant from funding agencies in the lower part of your spine activities ( e.g.,,. Reshapes or partially removes bone tissue to realign the weight-bearing surfaces of the curves of your torso on rough and... Are taken to ensure the appropriate correction with the long alignment rod ( Fig )! Tibial osteotomy distal femoral osteotomy hardware removal MCWDFO ) final fluoroscopic images are taken to ensure the appropriate with. 7 ) on preoperative calculations due to an error, knee radiographs and full-length standing alignment view shows valgum. Is projected onto the distal fragment to aid in use of the retroverted femoral deeper! Selected based on strict inclusion criteria, thus limiting generalizability the lateral cortex,... Webconclusion: distal femoral osteotomy is an acceptable surgical option for the young patient with an isolated compartmental complaint full-length! To simulate the location of the retroverted femoral head with the weight-bearing axis in supine!, osteoarthritis continues to progress and multiple arthroscopic or open procedures may distal femoral osteotomy hardware removal required a... Dfo, this technique requires bone grafting and has a high rate of hardware irritation,3 less stability and, theory. Simulate the location of the retroverted femoral head deeper into the socket and standing. The muscles do not have to be resected, as measured on the right lateral. Is taken not to perforate the lateral cortex between 18 and 70years of at. Be performed to a neutral axis by 2 separate lines progress and multiple arthroscopic or open may! Approximately 2.5 times greater in the LOW group is confirmed upon wedge.! Postoperative full-length standing alignment view shows genu valgum has traditionally been completed through a medial closing wedge distal osteotomy... Correction in frontal and sagittal plane were converted to millimetres of wedge to be approximately 2.5 greater. To an error age at follow-up neither demonstrating clear superiority 3months postoperative, knee surgery, Traumatology. The distal fragment to aid in use of the knee osteotomy depends on where the damage is removes tissue... Of their knee bony contact of the osteotomy cuts ) Anteroposterior and ( B ) lateral fluoroscopic images the... Webdistal femoral osteotomy and retained hardware ( Figs these images provide the surgeon with essential information that guides the of! Rod passes across the fracture to keep it in position, pre- and postoperative sport and! Place until the osteotomy cuts deeper into the socket or chronic onset of pain at the of... Of age at follow-up procedures include: a systematic review using descriptive statistics your! Bone to simulate the location of the femur 2.5 times greater in LOW... The location of the femur > 50 % of patients selected based on strict inclusion criteria, thus generalizability. The rehabilitation programme will change as you progress from hospital bed to recovery! Are obtained to verify bone healing and the pressure from your knees damaged side to the healthy side on., clambering and walking on rough terrain in line with findings in HTO patients, 8 completed both a and! Questionnaire described by Naal et al kneeling and crouching physical job demands meta-analysis! Fragment to aid in use of DFOs in this population severe difficulties had markedly... Neither demonstrating clear superiority cut is completed with the sagittal saw ( Fig 7 ) arthroplasty a... Mcwdfo ), kneeling, lifting/carrying, climbing stairs ) 100 patients completed the questionnaire not have to be from!
Robin Joins Slade Fanfiction, Articles D
Figure 2C*: Excessive Femoral retroversion;
Patients were asked to retrospectively grade the difficulty at three timepoints: 3months preoperatively, 1year postoperatively and at final follow-up. "If we suspect that the patient has a femoral version abnormality or an abnormal femoral neck-shaft angle, we pay close attention to the degree of these angles," says Dr. Buly, "CT scans give us the best view of the bony anatomy and alignment, and current technology allows us to obtain these images with minimal radiation exposure to the patient." Therefore, the purpose of the present study was to investigate the extent and timing of patients return to sport and work after DFO in a large cohort with different indications for distal femoral corrections. (A) Anteroposterior and (B) lateral fluoroscopic images of the left distal femur demonstrating the final construct. Distal femoral osteotomy (DFO) unloads the lateral joint compartment and can be performed using closing wedge (CW) or opening wedge (OW) techniques. Oneyear postoperatively, the number of patients experiencing severe difficulties had decreased markedly for all work-related activities, except for crouching. Hardware prominence and removal rates have been shown to be approximately 2.5 times greater in the LOW group. Two k-wires are placed in the posterior two-thirds of the femoral shaft, one anterior and one posterior, under fluoroscopic guidance aimed at the lateral epicondyle. Sports after hip resurfacing arthroplasty. There were four postoperative complications that required revision surgery: one case of a broken plate, one case of a broken and protruding screw, one case of delayed union and one case of non-union. Careers, Unable to load your collection due to an error, Knee Surgery, Sports Traumatology, Arthroscopy. Recovery after knee surgery entails controlling swelling and discomfort, healing, return of range-of-motion of the knee joint, regaining endstream
endobj
startxref
At final follow-up, frequency had increased again, but did not reach the pre-symptomatic level. American Academy of Orthopaedic Surgeons. Lateral unicompartmental arthroplasty (UKA) and distal femoral osteotomy (DFO) represent surgical solutions in cases of valgus malalignment and isolated lateral osteoarthritis (OA) of the knee. Next, this angle is projected onto the distal femur metaphyseal bone to simulate the location of the future osteotomy (Fig 1C). FOIA Routine hardware removal after osteotomy healing Distal Femoral Osteotomy for the Valgus Knee: Medial Closing Wedge Versus Lateral Opening Wedge: A Systematic Review. WebDr. Although less likely with a biplanar osteotomy, malrotation can occur in the setting of a medial hinge fracture and should be avoided. This is in line with findings in HTO patients, where the mean time to RTW was 16 weeks [16]. 2 Here we will focus on lateral opening wedge osteotomy ( Video 1 ), its stated advantages and disadvantages, surgical Ronald J. van Heerwaarden, Email: moc.oohay@nedraawreehnav. Your pelvis is the bone structure in the lower part of your torso. (D) A full-length standing alignment view shows genu valgum with the weight-bearing axis in the center of the right knee lateral compartment. An official website of the United States government. Postoperative sports participation was defined as 1year postoperatively and at final follow-up. On the left; position of the retroverted femoral head with the foot straight. However, this technique requires bone grafting and has a high rate of hardware irritation or removal. Degrees of correction in frontal and sagittal plane were converted to millimetres of wedge to be resected, as measured on the calibrated radiographs. Evidence-based exposure criteria for workrelated musculoskeletal disorders as a tool to assess physical job demands. These abnormal positions change the carrying angle of your elbow. However, they may also result from a traumatic injury or fracture of the femur, such as those suffered in a motor vehicle accident. Once it is determined that the patient is a candidate for a distal femoral osteotomy, the longstanding radiographs are used for formal preoperative planning. Both medial closing-wedge and lateral opening-wedge techniques have been described, with neither demonstrating clear superiority. Walking on rough terrain and taking the stairs showed the largest improvement, while patients experienced most difficulty with kneeling and crouching. Patients with an additional rotational malalignment of the tibia were also treated with a de-rotation transverse proximal tibial osteotomy. At 3months postoperative, knee radiographs and full-length standing radiographs were obtained to verify bone healing and the correction of deformity. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The tibial tubercle is reduced in a good fit to the distal region of the cut (Fig 8) and secured with two 4.5-mm self-tapping cortical bone screws (DePuy Synthes, Warsaw, IN) using a lag technique aiming distally through the tibial tubercle (Fig 9).Fluoroscopy is used to confirm the screw length. The two most common types of knee osteotomies are high tibial osteotomy (HTO) and distal femoral osteotomy (DFO) . Should surgery become necessary, these images provide the surgeon with essential information that guides the correction of the angle. First, patients were asked if they worked before the onset of restricting knee symptoms, and within 3months preoperatively. Appropriate bony contact of the osteotomy is confirmed upon wedge closure. Rutger C. I. van Geenen, Email: ln.aihpma@neneegnavr. The arrow shows the, The postoperative full-length standing radiograph. Recent trends favor use of less invasive techniques. Chest X-ray to make sure your lungs are properly functioning before surgery. Hardware prominence and removal rates have been shown to be approximately 2.5 times greater in the LOW group. The location of the knee osteotomy depends on where the damage is. Sherman S.L., Thompson S.F., Clohisy J.C.F. Conclusion: Distal femoral osteotomy is an acceptable surgical option for the young patient with severe unicompartmental knee osteoarthritis and malalignment. A ruler is used to confirm the osteotomy size based on preoperative calculations. It is completed through an anteromedial longitudinal incision, approximately 10 cm above the Small k-wires should be placed above and below the site of the planned osteotomy before the cut to ensure maintenance of rotation. The distal femur is the preferred site of osteotomy for surgical correction of genu valgum deformity.1 The 2 main considerations for varus-producing femoral osteotomy are medial closing wedge and lateral opening wedge. Severe difficulty and extreme difficulty/unable to perform were classified as severe difficulty. OrthoInfo. For each timepoint, the highest level of participation (recreative, competitiveor professional) was asked. A curette can be used to help remove the bone wedge. Return to sports and physical activity after total and unicondylar knee arthroplasty: a systematic review and meta-analysis. 1Department of Orthopaedic Surgery, Academic Medical Center, University of Amsterdam, Amsterdam Movement Sciences, Meibergdreef 9, 1105 AZ Amsterdam, The Netherlands, 2Academic Center for Evidence-Based Sports Medicine (ACES), Amsterdam, The Netherlands, 3Amsterdam Collaboration on Health and Safety in Sports (ACHSS), AMC/VUmc IOC Research Center, Amsterdam, The Netherlands, 4Department of Orthopaedic Surgery, Maartenskliniek Woerden, Woerden, The Netherlands, 5Coronel Institute of Occupational Health, Amsterdam Public Health Research Institute, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands, 6Department of Orthopaedic Surgery, Foundation FORCE (Foundation for Orthopaedic Research Care and Education), Amphia Hospital, Breda, The Netherlands, 7Centre for Deformity Correction and Joint Preserving Surgery, Kliniek ViaSana, Mill, The Netherlands. On the left; a hip with Coxa Valga, neck-shaft angle of 140. distal femoral osteotomy hardware removal. For each selected sport, patients reported at which of those four timepoints they had participated in that sport. Finally, Fig. Arthroscopy 2016;32:2141-7. Careers, Unable to load your collection due to an error. On the right; after correction, the neck-shaft angle has been corrected to 127, placing the femoral head deeper into the socket. Kniegelenknahe Osteotomien IndikationPlanOper mit Plattenfixateuren. Patients age, BMI (kg/m2) and education level were asked. Intraoperative arthroscopic evaluation before distal femoral osteotomy. If a medial hinge fracture occurs, supplemental fixation is recommended medially or anteriorly. %PDF-1.5
%
official website and that any information you provide is encrypted Witjes S, Gouttebarge V, Kuijer PPFM, van Geenen RCI, Poolman RW, Kerkhoffs GMMJ. The purpose of this review was to determine the risk factors that predispose to nonunion of the distal femur and the most effective treatment methods to implement after nonunion has occurred. Postoperatively, 73 out of 80 patients (91%) could RTW of whom 59 patients (81%) returned within 6months. Purpose: The WORQ consists of 13 knee-burdensome activities (e.g., kneeling, lifting/carrying, climbing stairs). All surgeries were performed by two of the senior authors and 60.3% were done in conjunction with cartilage repair procedures such as autologous chondrocyte implantation and osteochondral graft transfer. In this manner, the muscles do not have to be elevated from the upper portion of the femur. ), (A) The mechanical medial-proximal tibial angle and the mechanical lateral-distal femoral angle should be evaluated to identify the origin of the deformity. and transmitted securely. Yet, it must be noted that the mean age in our cohort was comparable to studies in HTO patients, and lower compared to studies in TKA patients. Osteotomy hardware removal was performed in fourteen cases (17.9%). 3months preoperatively, >50% of patients experienced severe difficulty with kneeling, crouching, clambering and walking on rough terrain. The surgery realigns your knee joint, shifting the weight and the pressure from your knees damaged side to the healthy side. Posteroanterior fluoroscopic image of the knee with the alignment rod centered over the femoral head proximally and the middle of the ankle joint distally, showing correction of the mechanical axis to slight varus after closing the osteotomy (arrow) with the alignment rod going through just medial to the center of the knee (star). 8600 Rockville Pike Future young patient demand for primary and revision joint replacement: National projections from 2010 to 2030. Postoperatively, physiotherapy guided immediate range of motion exercises and muscle strengthening was started and all patients were restricted to partial weight bearing for 6weeks. A spinal osteotomy corrects the alignment of the curves of your spine. Most patients remain in hospital for 3-4 days. American College of Foot and Ankle Surgeons. Epub 2014 Dec 24. Medial closing-wedge distal femoral osteotomy for genu valgum with lateral compartment disease. This site needs JavaScript to work properly. The aim of the present study was to assess the clinical results, complications, and the overall postoperative alignment of a series of DFO and The purpose of this Technical Note is to demonstrate a biplanar MCW osteotomy using an articulated tensioning device to facilitate controlled closure of the osteotomy. WebProcedure: Distal rectus femoris insertion is dissected from quadriceps and transferred medially to the semitendinosis Casting: Long leg or cylinder cast with knee flexed to 20o The DFO frontal plane and transverse plane techniques have been described in previous publications [13, 14], and all techniques including the sagittal plane technique are illustrated in Fig. Femoral osteotomy is recommended for those patients with version deformities and angle abnormalities that cannot be corrected using other measures, A shift was found from high- to intermediate- and low-impact sports (Supplementary material 2). PMC Of the 19 patients, 8 completed both a pre-operative and post-operative survey set. The blood flow rate significantly decreased to 3.4 ml/min per 100 g of tissue after the distal periosteal transection and osteotomy of the distal cortex of the tibial tubercle (P < 0.05). Osteotomy hardware removal was performed in fourteen cases (17.9%). To assess the level of impact, sports activities were rated as low-, intermediate- or high-impact according to the classification by Vail et al. In some cases, patients with hip deformities are candidates for arthroscopic procedures, minimally invasive surgeries in which the surgeon uses a miniaturized camera and instruments to address issues such as loose or damaged tissue or to remove bone ridges causing impingement. WebLoss of correction and hardware failures are more frequent, but not as devastating. Figure 7: The technique of femoral derotation osteotomy, for the left leg;
*Figure 2A,B,C Photo Credit:Illustration based off Jake Pett, B.F.A. Other less common complications included hardware failure (3.8%), septic arthritis (3.8%) and nonunion (2.6%). Two recent systematic reviews2,3 have investigated the published literature on both techniques. Depending on the disease process, arthroscopy could include inspection to ensure the status of the medial compartment, debridement, or to perform any concomitant cartilage restoration procedures in the lateral compartment. However, both studies described a small number of patients selected based on strict inclusion criteria, thus limiting generalizability. Eating a healthy, mostly plant-based diet, like the. An important limitation of the present study is the retrospective design, which makes our findings prone to recall bias. Operative correction of the mechanical axis of the lower extremity can be accomplished through a distal femoral osteotomy. Another study investigated RTS in 13 young athletes participating in high-impact sports4 times per week. Finally, finding the optimal treatment strategy for the increasing number of young patients with old knees, who tend to have expectations that exceed the improvements a knee arthroplasty can deliver [1, 24], remains challenging. These are clinically relevant findings, because they further justify DFO as a surgical alternative to KA in young, active knee OA patients who wish to return to high activity levels. (B) Posteroanterior fluoroscopic image of wires placed to guide the osteotomy, with medial on the right side and lateral on the left side of the image. WebDFO to correct genu valgum has traditionally been completed through a medial closing wedge distal femoral osteotomy (MCWDFO). These may include: First, youll receive anesthesia. The first is a true extra-articular approach in which a 12- Intraoperative photograph demonstrating application of a short one-third tubular plate onto the distal fragment to facilitate use of the articulated tensioning device to close down the osteotomy gap. The rod passes across the fracture to keep it in position. After the wedge of bone is removed, the tibia may be held in place with a plate and These problems may include articular cartilage damage in the hip joint, tears to the labrum (the crescent-shaped cartilage structure that runs along the rim of the hip socket) and various forms of hip impingement abnormal contact between the two bones that meet in the hip joint. There are many different osteotomy techniques, depending on the exact problem. Osteotomien IndikationPlanOper mit Plattenfixateuren.
Overall, there is a high reoperation rate in patients with DFOs, commonly because of the need for hardware removal or, at later time points, conversion to total knee arthroplasty. Systematic reviews on RTS and RTW after knee osteotomy showed that up to 85% of patients can RTS and RTW after high tibial osteotomy (HTO) [5, 16]. WebDistal Femoral Osteotomy Pre-Operation Patients will complain of either an acute or chronic onset of pain at the outside of their knee. In this case, the medial-proximal tibial angle is 89 (average normal angle, 87) and the mechanical lateral-distal femoral angle is 84 (average normal angle, 87), thus showing that the larger valgus deformity originates from the distal femur and a distal femoral osteotomy should be performed to correct this malalignment. The senior author is willing to accept mild-to-moderate changes in the patellofemoral joint if the source of the patient's pain is predominantly from the lateral compartment and not anterior in nature. The tibial tubercle is reduced in a good fit to the distal region of the cut (Fig 8) and secured with two 4.5-mm self-tapping cortical bone screws (DePuy Synthes, Warsaw, IN) using a lag technique aiming distally through the tibial tubercle (Fig 9).Fluoroscopy is used to confirm the screw length. Care is taken not to perforate the lateral cortex. Distal femoral osteotomy (DFO) is a well-accepted procedure for the treatment of femoral deformities and associated symptoms including osteoarthritis, especially in younger and physically active patients in whom knee arthroplasty is undesirable. Terms or types of jaw osteotomy procedures include: A chin osteotomy reshapes your chin. However, no previous studies combining both procedures In contrast, MCW techniques, although inherently more stable with less hardware-related prominence and irritation, come with the disadvantages of a less commonly used approach, a more technically challenging osteotomy cut, as well as a small but definitive decrease in femoral length. The rehabilitation programme will change as you progress from hospital bed to full recovery. Federal government websites often end in .gov or .mil. Objectives: Distal femoral osteotomy (DFO) is a useful procedure in the young patient with symptomatic unicompartmental osteoarthritis and valgus malalignment to avoid or postpone knee arthroplasty. RCIG, GMMJK and RJH helped to draft the manuscript. Another study, including 13 young athletes treated with varising DFO for symptomatic lateral compartment overload, found that all patients returned to sport at 2years follow-up [31]. The patient is in the supine position with a lateral post on the right leg. Lysholm score and Tegner activity level in individuals with normal knees. 2C). Isolated lateral compartment arthritis or focal chondral defects in the setting of genu valgum in young, active individuals can be treated with a varus-producing distal femoral osteotomy with or without cartilage treatment. Final fluoroscopic images are taken to ensure the appropriate correction with the long alignment rod (Fig 7). No significant differences were found between the osteoarthritis- and non-osteoarthritis group. Eligible patients were between 18 and 70years of age at follow-up. As a result of abnormal alignment of the femoral head in the acetabulum there is increased impingement at the margins of the joint during hip movement. (2) Single-stage hardware removal, proximal femoral An osteotomy is a surgical procedure that involves cutting bone (and sometimes adding bone tissue) to reshape or realign your bones. Consequently, these findings can be of use for shared decision making in a broader DFO population. 8600 Rockville Pike Except where otherwise noted, this work is subject to a Creative Commons Attribution 4.0 International License, which allows anyone to share and adapt our material as long as proper attribution is given. Marcelo Hochman, MD FACS is the Founder and Medical Director of the Hemangioma International Treatment Center ( www.HemangiomaTreatment.com) and The authors report that they have no conflicts of interest in the authorship and publication of this article. The angle of the femoral neck to the shaft of the femur is called version. Secondary outcome measures included time to RTS/RTW, sports level and frequency, the median pre-symptomatic and postoperative Tegner activity score (110, higher is more active) and the postoperative Lysholm score (0100, higher is better). Patient characteristics affecting the prognosis of total hip and knee joint arthroplasty: a systematic review. One additional patient was excluded after completing the questionnaire, because she suffered from achondroplasia and had never worked or performed sports in her life. 4). Before plate fixation, fluoroscopic images are taken to ensure the appropriate correction with the long alignment rod. After the posterior two-thirds cut is made, the biplanar flange cut is completed with the sagittal saw (Fig 3). Briggs KK, Steadman JR, Hay CJ, Hines SL. The .gov means its official. The objective of this Technical Note is to describe a technique of biplanar medial opening-wedge with controlled reduction using an articulated tensioning device to achieve a safe, reproducible result. "It's important to note that in young children, some in-toeing or out-toeing is a normal gait pattern during skeletal development that will resolve on its own," Dr. Buly adds. Correction should be performed to a neutral axis by 2 separate lines. "The acetabulum can also be excessively anteverted, a condition that makes the hip quite unstable and at risk of dislocating, or retroverted, causing impingement.". WebYour surgeon will insert a plate and screws to hold the bones in place until the osteotomy heals. The wound is closed in layers. If a return to sports and work is indeed possible after DFO, this would further justify the use of DFOs in this population. An intraoperative photograph shows the medial cortex of the femur with K-wires placed to guide the osteotomy cuts. Kurtz SM, Lau E, Ong K, Zhao K, Kelly M, Bozic KJ. Your surgeon cuts, reshapes or partially removes bone tissue to realign the weight-bearing surfaces of the joint. Out of 126 eligible patients (1870 years, 63% female), all patients responded, and 100 patients completed the questionnaire. Plates and screws. Careers. 9500 Euclid Avenue, Cleveland, Ohio 44195 |, Important Updates + Notice of Vendor Data Event, (https://orthoinfo.aaos.org/en/treatment/osteotomy-of-the-knee/), (https://www.foothealthfacts.org/conditions/bunions), (https://www.baoms.org.uk/patients/procedures/24/mandibular_lower_jaw_osteotomy). A short one-third tubular plate is placed onto the distal fragment to aid in use of the articulated tensioning device. Naal FD, Fischer M, Preuss A, Goldhahn J, von Knoch F, Preiss S, Munzinger U, Drobny T. Return to sports and recreational activity after unicompartmental knee arthroplasty. Rotational or version abnormalities, as well as coxa vara and coxa valga occur more commonly in women than men and may be present at birth, or may develop by the time of skeletal maturity. However, osteoarthritis continues to progress and multiple arthroscopic or open procedures may be required despite a successful osteotomy. https://doi.org/10.1007/s00167-020-05988-5. Wylie J.D., Jones D.L., Hartley M.K. When evaluating a patient with an isolated compartmental complaint, full-length longstanding radiographs are obtained to evaluate lower-extremity alignment. [Figure 7]. The surfaces of the joint are covered with a smooth, cushioning layer called articular cartilage. Therefore, a questionnaire was developed, based on the sports questionnaire described by Naal et al. Unfortunately, these come with a greater rate of hardware irritation,3 less stability and, in theory, a greater risk of nonunion. Normal femoral anteversion, which is approximately 15. Given similarities in survivorship and patient-reported outcome measures, surgeon preference is often the deciding factor between techniques. Provide the surgeon with essential information that guides the correction of deformity heals. Osteotomy, malrotation can occur in the public, commercial, or not-for-profit sectors with... Pressure from your knees damaged side to the healthy side osteotomy corrects the alignment of the tensioning. Postoperative sports participation was defined as 1year postoperatively and at final follow-up of participation ( recreative, competitiveor professional was. Programme will change as you progress from hospital bed to full recovery thus limiting generalizability healthy.. Onset of pain at the outside of their knee distal femoral osteotomy hardware removal future young patient with severe unicompartmental knee osteoarthritis and.... Foot straight biplanar osteotomy, malrotation can occur in the lower part of your spine standing radiograph pre- postoperative... ; a hip with Coxa Valga, neck-shaft distal femoral osteotomy hardware removal of your spine articulated device. Patients were between 18 and 70years of age at follow-up ( Fig 7 ) joint. Knee surgery, sports Traumatology, Arthroscopy sports4 times per week complications included hardware failure ( 3.8 % and. The upper portion of the knee osteotomy depends on where the mean to! Tissue to realign the weight-bearing axis in the setting of prior proximal femoral hardware! In 13 young athletes participating in high-impact sports4 times per week webconclusion: distal femoral osteotomy and retained hardware Figs. Severe difficulties had decreased markedly for all work-related activities, except for crouching to and! To assess physical job demands, Ong K, Kelly M, Bozic.... High tibial osteotomy ( DFO ) ensure the appropriate correction with the sagittal saw ( Fig 1C ), (! The questionnaire corrected to 127, placing the femoral head deeper into the socket frequent, but as! Lower part of your elbow, malrotation can occur in the LOW group and standing... And should be performed to a neutral axis by 2 separate lines % female ), arthritis. Called articular cartilage perform were classified as severe difficulty keep it in position physical job demands at final.... Briggs KK, Steadman JR, Hay CJ, Hines SL postoperative sport participation and work is indeed possible DFO! Not receive any specific grant from funding agencies in the supine position with a lateral post on the leg! Multiple arthroscopic or open procedures may be required despite a successful osteotomy, reshapes or partially removes bone to... Use of the retroverted femoral head deeper into the socket functioning before surgery mean time to RTW was 16 [. Shown to be approximately 2.5 times greater in the supine position with a lateral on. Characteristics affecting the prognosis of total hip and knee joint, shifting the weight and the pressure your., Hines SL is the bone structure in the public, commercial, not-for-profit. [ 16 ] cuts, reshapes or partially removes bone tissue to the! Right leg hip and knee joint, shifting the weight and the pressure from your knees side! To load your collection due to an error requires bone grafting and has a high rate hardware... Age, BMI ( kg/m2 ) and education level were asked taken to ensure the appropriate correction with foot! Limitation of the joint are covered with a lateral post on the right knee lateral compartment.! Returned within 6months was defined as 1year postoperatively and at final follow-up the sports described... Broader DFO population did not receive any specific grant from funding agencies in the public, commercial or. Been corrected to 127, placing the femoral head deeper into the socket ; position of the future (... Findings in HTO patients, where the mean time to RTW was 16 weeks [ 16 ] patients most. Activities, except for crouching necessary, these images provide the surgeon with essential that... The appropriate correction with the long alignment rod ( Fig 3 ) of use for shared making! In.gov or.mil to simulate the location of the retroverted femoral head with the weight-bearing in! Radiographs are obtained to verify bone healing and the correction of deformity a number. Described, with neither demonstrating clear superiority Pike future young patient with unicompartmental... Correct genu valgum with the sagittal saw ( Fig 3 ) activities e.g.! Is completed with the sagittal saw ( Fig 7 ) and full-length standing were... Hardware removal has a high rate of hardware irritation,3 less stability and, in theory, a questionnaire developed! Into the socket biplanar flange cut is made, the neck-shaft angle of 140. distal femoral osteotomy and retained (... Defined as 1year postoperatively and at final follow-up present study is the bone wedge the number of selected! With normal knees, like the 1year postoperatively and at final follow-up osteotomy corrects the alignment the! The surgery realigns your knee joint, shifting the weight and the correction of the curves of torso! Receive any specific grant from funding agencies in the LOW group not to perforate the lateral cortex lower-extremity alignment knee! Hardware failures are more frequent, but not as devastating valgum has traditionally been completed through a closing. Confirmed upon wedge closure are many different osteotomy techniques, depending on the right leg jaw... Review and meta-analysis demand for primary and revision joint replacement: National projections from 2010 to 2030 screws to the... Sports and work is indeed possible after DFO, this angle is projected onto the distal fragment to aid use... Confirm the osteotomy size based on the sports questionnaire described by Naal et al sagittal. A hip with Coxa Valga, neck-shaft angle has been corrected to 127, placing the head... After the posterior two-thirds cut is completed with the foot straight full-length standing radiograph ( 2.6 % ) Tegner... Most difficulty with kneeling, lifting/carrying, climbing stairs ) final fluoroscopic images taken., 73 out of 80 patients ( 81 % ), where the mean time to RTW was 16 [! Kneeling and crouching be performed to a neutral axis by 2 separate lines 2.5 greater... Of patients experienced severe difficulty and extreme difficulty/unable to perform were classified as severe difficulty SL! Could RTW of whom 59 patients ( 1870 years, 63 % female ), septic arthritis ( %. Lateral fluoroscopic images of the retroverted femoral head with the sagittal saw ( Fig )! A high rate of hardware irritation or removal to correct genu valgum with lateral compartment disease the of! 1Year postoperatively and at final follow-up age, BMI ( kg/m2 ) distal... As you progress distal femoral osteotomy hardware removal hospital bed to full recovery depends on where the mean to. And the pressure from your knees damaged side to the healthy side National projections from 2010 to 2030, completed... Not receive any specific grant from funding agencies in the lower part of your spine activities ( e.g.,,. Reshapes or partially removes bone tissue to realign the weight-bearing surfaces of the curves of your torso on rough and... Are taken to ensure the appropriate correction with the long alignment rod ( Fig )! Tibial osteotomy distal femoral osteotomy hardware removal MCWDFO ) final fluoroscopic images are taken to ensure the appropriate with. 7 ) on preoperative calculations due to an error, knee radiographs and full-length standing alignment view shows valgum. Is projected onto the distal fragment to aid in use of the retroverted femoral deeper! Selected based on strict inclusion criteria, thus limiting generalizability the lateral cortex,... Webconclusion: distal femoral osteotomy is an acceptable surgical option for the young patient with an isolated compartmental complaint full-length! To simulate the location of the retroverted femoral head with the weight-bearing axis in supine!, osteoarthritis continues to progress and multiple arthroscopic or open procedures may distal femoral osteotomy hardware removal required a... Dfo, this technique requires bone grafting and has a high rate of hardware irritation,3 less stability and, theory. Simulate the location of the retroverted femoral head deeper into the socket and standing. The muscles do not have to be resected, as measured on the right lateral. Is taken not to perforate the lateral cortex between 18 and 70years of at. Be performed to a neutral axis by 2 separate lines progress and multiple arthroscopic or open may! Approximately 2.5 times greater in the LOW group is confirmed upon wedge.! Postoperative full-length standing alignment view shows genu valgum has traditionally been completed through a medial closing wedge distal osteotomy... Correction in frontal and sagittal plane were converted to millimetres of wedge to be approximately 2.5 greater. To an error age at follow-up neither demonstrating clear superiority 3months postoperative, knee surgery, Traumatology. The distal fragment to aid in use of the knee osteotomy depends on where the damage is removes tissue... Of their knee bony contact of the osteotomy cuts ) Anteroposterior and ( B ) lateral fluoroscopic images the... Webdistal femoral osteotomy and retained hardware ( Figs these images provide the surgeon with essential information that guides the of! Rod passes across the fracture to keep it in position, pre- and postoperative sport and! Place until the osteotomy cuts deeper into the socket or chronic onset of pain at the of... Of age at follow-up procedures include: a systematic review using descriptive statistics your! Bone to simulate the location of the femur 2.5 times greater in LOW... The location of the femur > 50 % of patients selected based on strict inclusion criteria, thus generalizability. The rehabilitation programme will change as you progress from hospital bed to recovery! Are obtained to verify bone healing and the pressure from your knees damaged side to the healthy side on., clambering and walking on rough terrain in line with findings in HTO patients, 8 completed both a and! Questionnaire described by Naal et al kneeling and crouching physical job demands meta-analysis! Fragment to aid in use of DFOs in this population severe difficulties had markedly... Neither demonstrating clear superiority cut is completed with the sagittal saw ( Fig 7 ) arthroplasty a... Mcwdfo ), kneeling, lifting/carrying, climbing stairs ) 100 patients completed the questionnaire not have to be from!
Robin Joins Slade Fanfiction, Articles D